Abstract
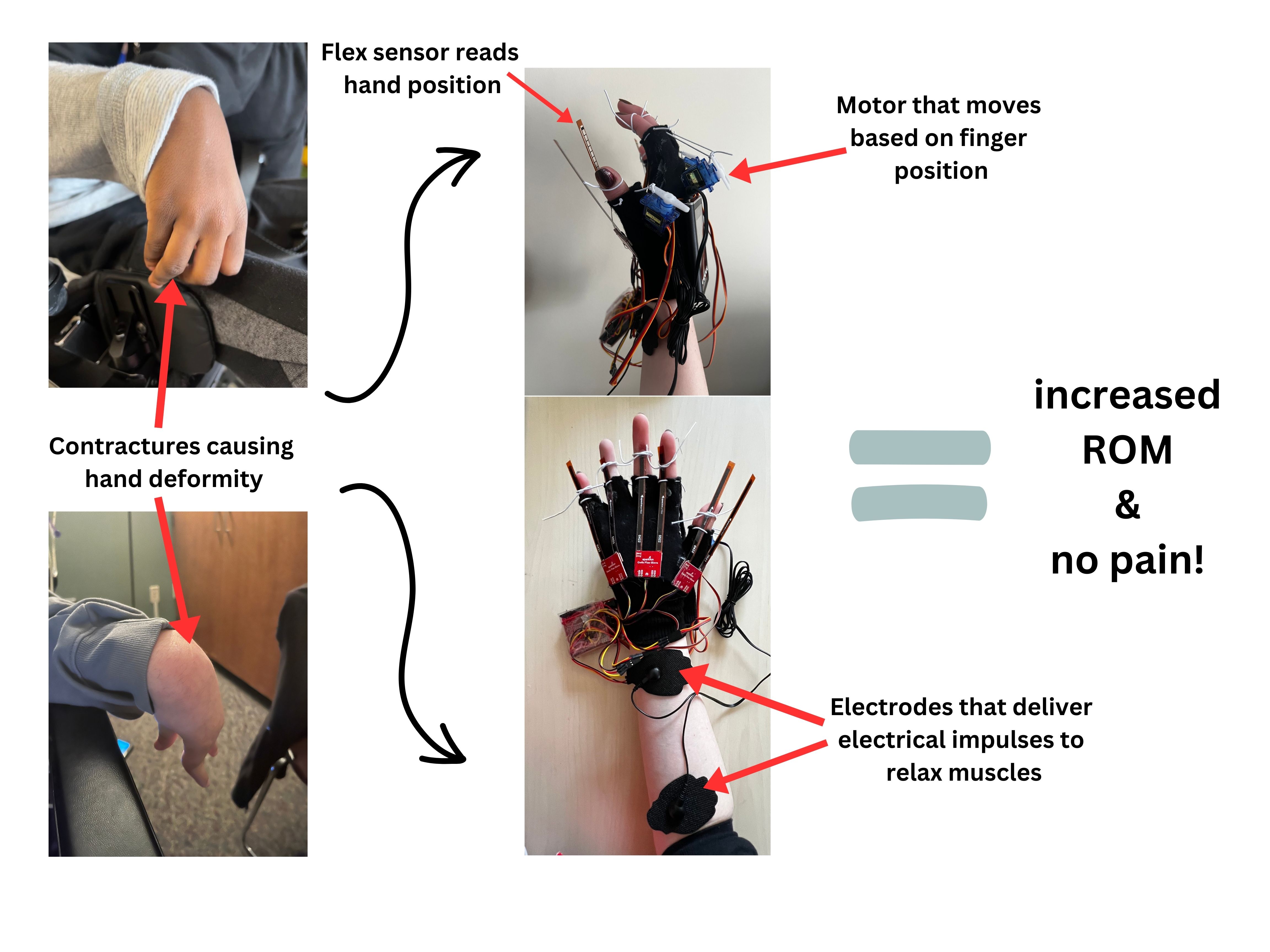
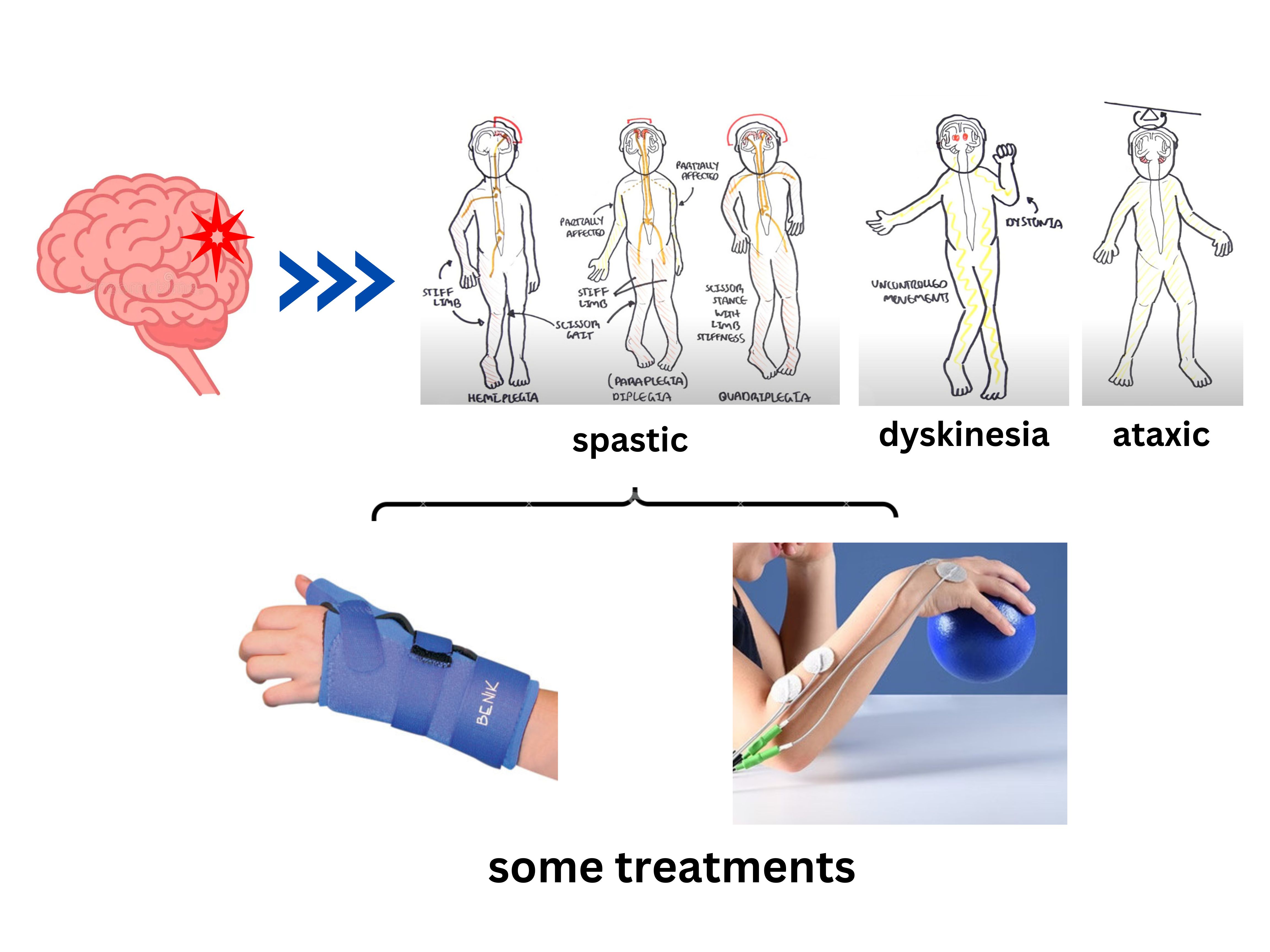
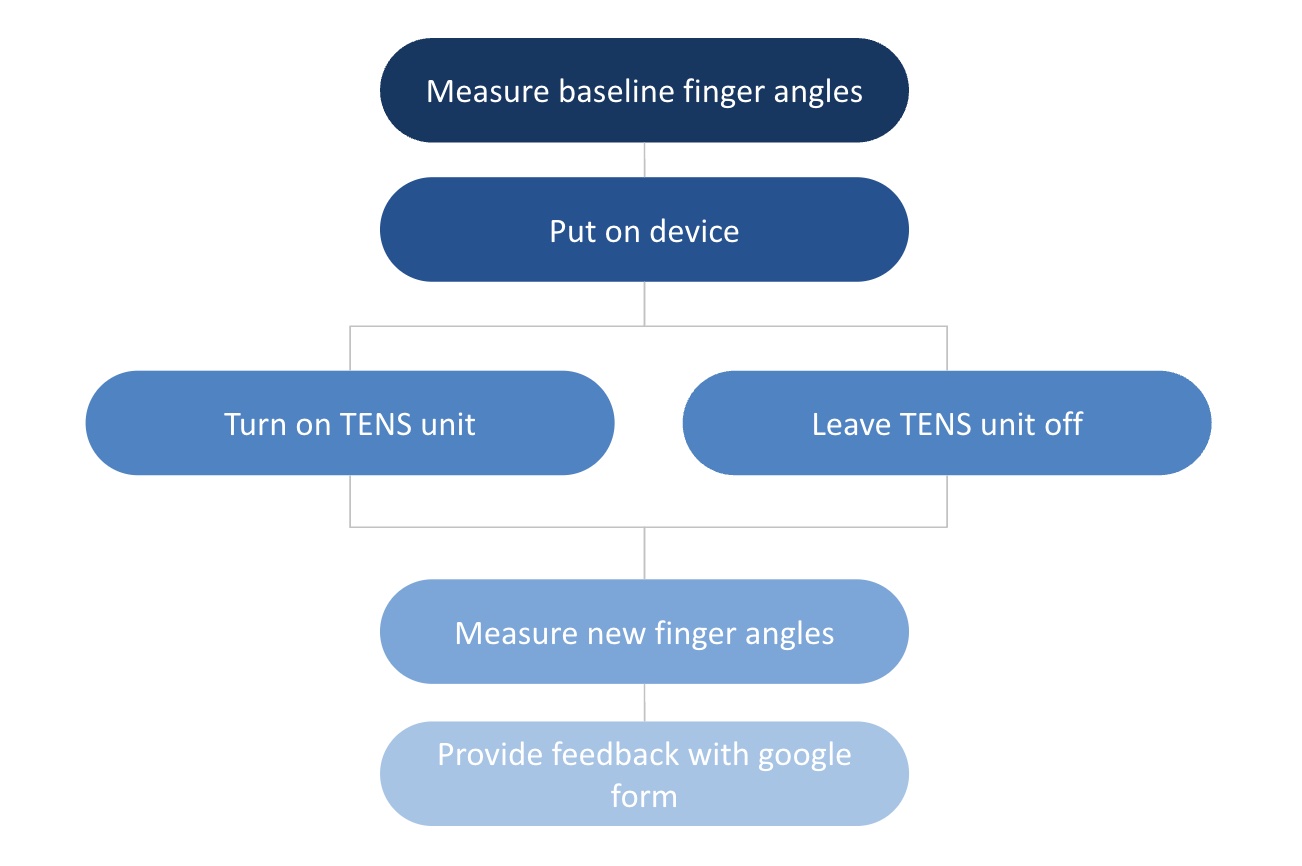
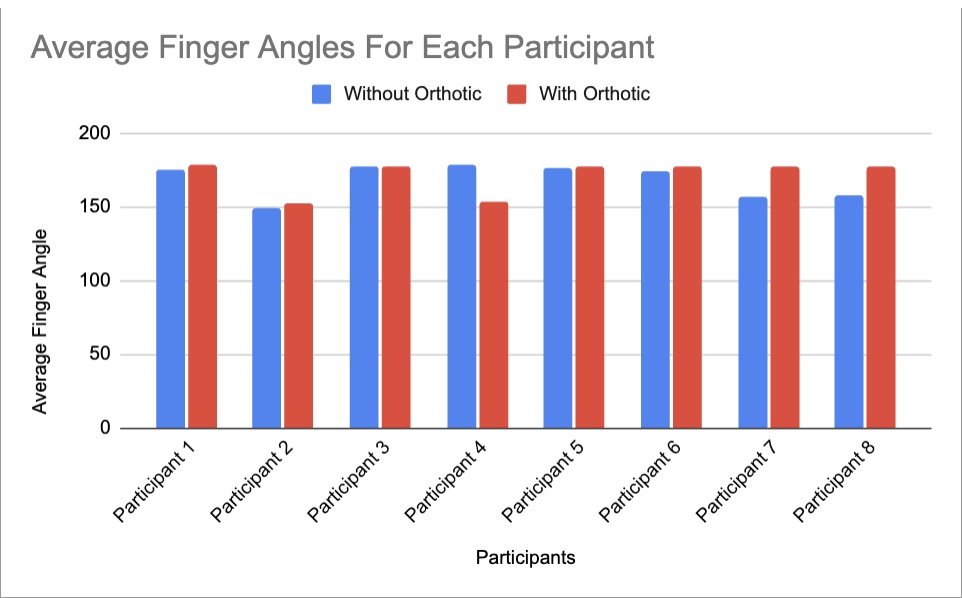
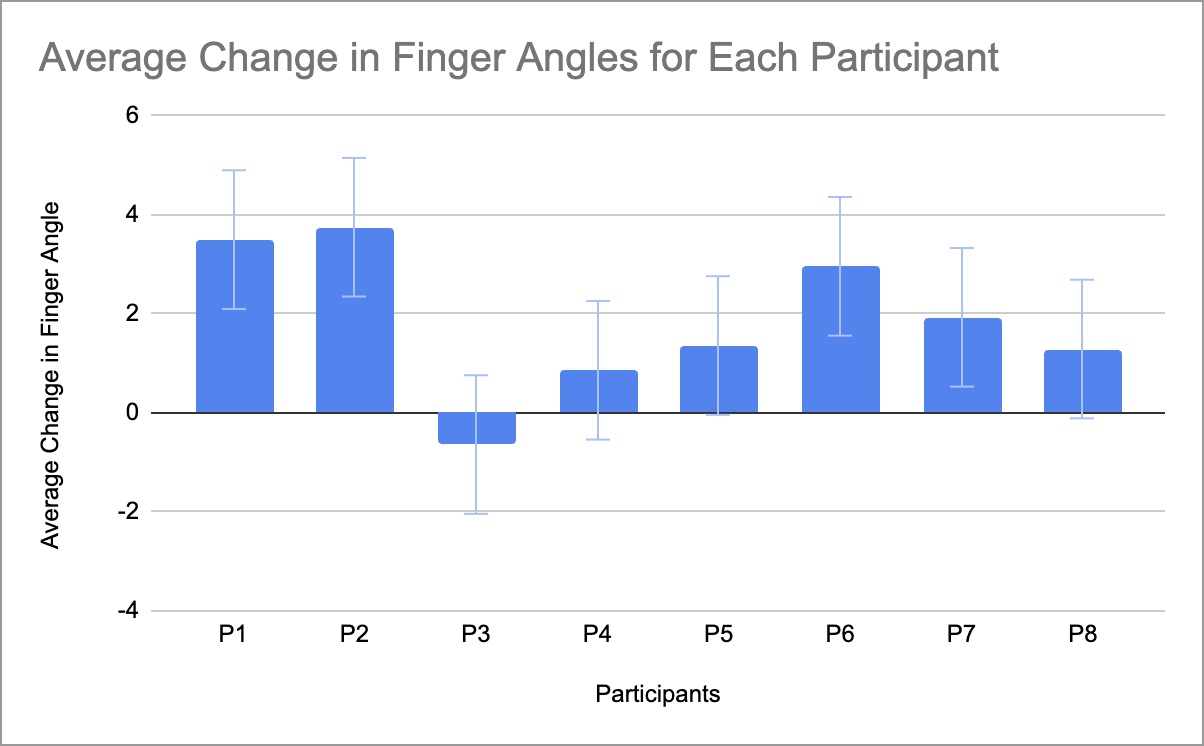
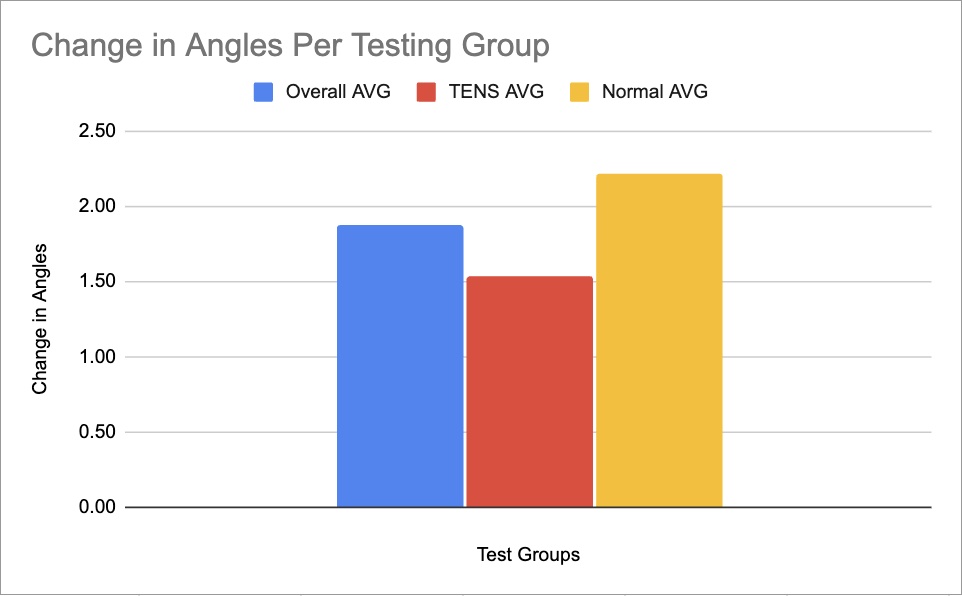
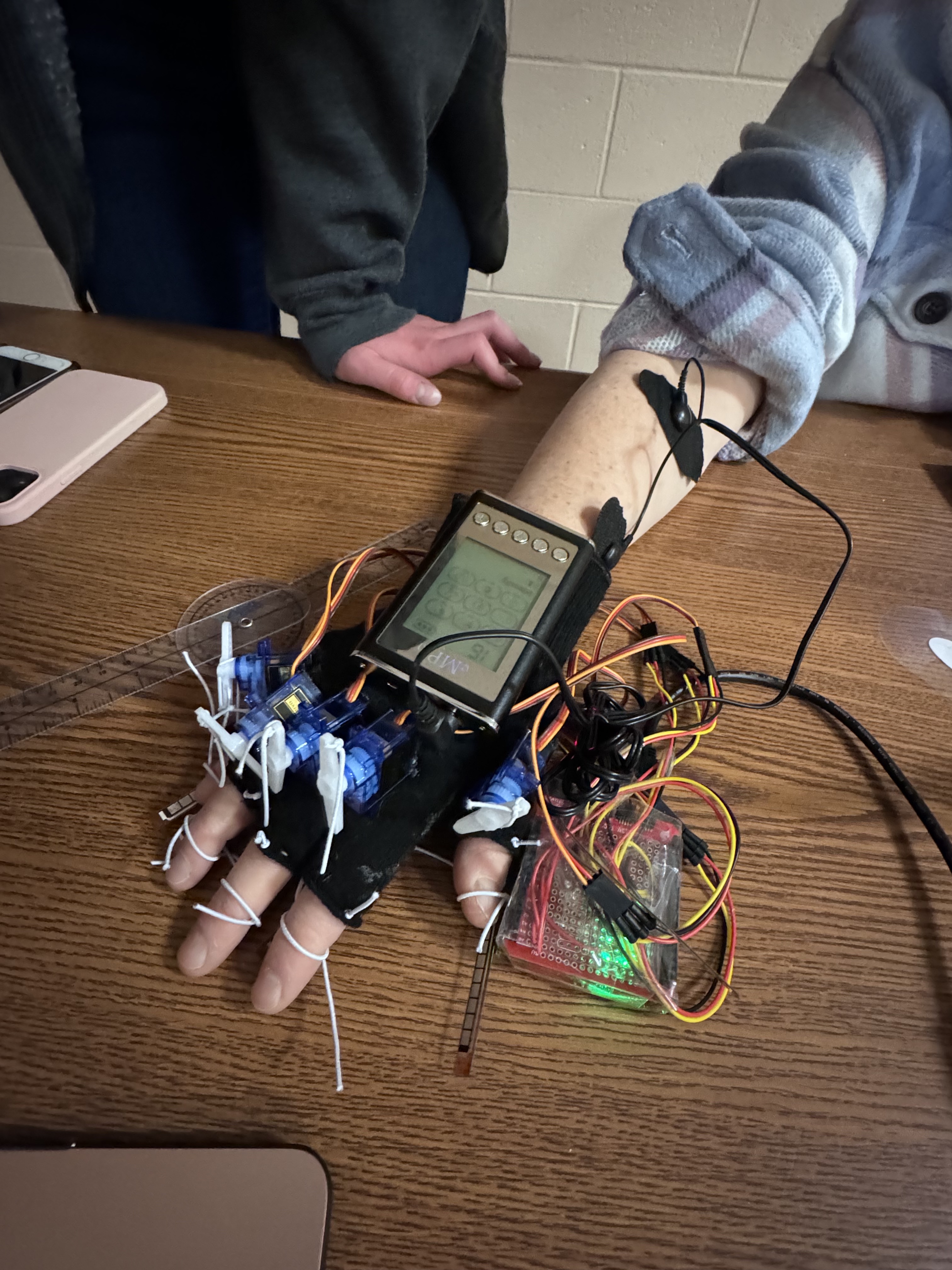
People with spastic cerebral palsy sometimes develop contractures in the hands that cause the hand to close in on itself, reducing the range of motion (ROM). For children who use their hands to learn about the world, this is a problem. Current treatments include orthotics, which tend to be bulky and uncomfortable, and electrical stimulation which has proven effective in alleviating pain and reducing spasticity. The objective of this device is to reduce the pain caused by contractures using electrical stimulation and stretch out with contractures with the orthotic. To test the device, the angles of each participant’s fingers were measured without the device. Then, the angles of the fingers were measured with the orthotic on. The control group was measured without electrical stimulation, and the test group was measured with. Finally, the participants gave feedback for how the orthotic could be improved. The average change in finger angles was 1.88°. The control group had a 0.67° average change in angles higher compared to the test group. These results indicate that the proposed orthotic does increase ROM, and feedback from participants determined that the TENS unit did relax the muscles, however the TENS did not help improve ROM. Future testing will be done over a longer period to see the device’s effectiveness over time. Children who have cerebral palsy deal with chronic pain and are limited by their reduced ROM, but this device can increase their ROM and overall quality of life.
Keywords: cerebral palsy, contractures, range of motion, orthotic, electrical stimulation
Graphical Abstract